

Sulfonylureas: Who is at risk?
A number of factors increase the likelihood of a sulfonylurea causing hypoglycaemia, especially in the elderly, and some of these risk factors are summarised in the diagram below: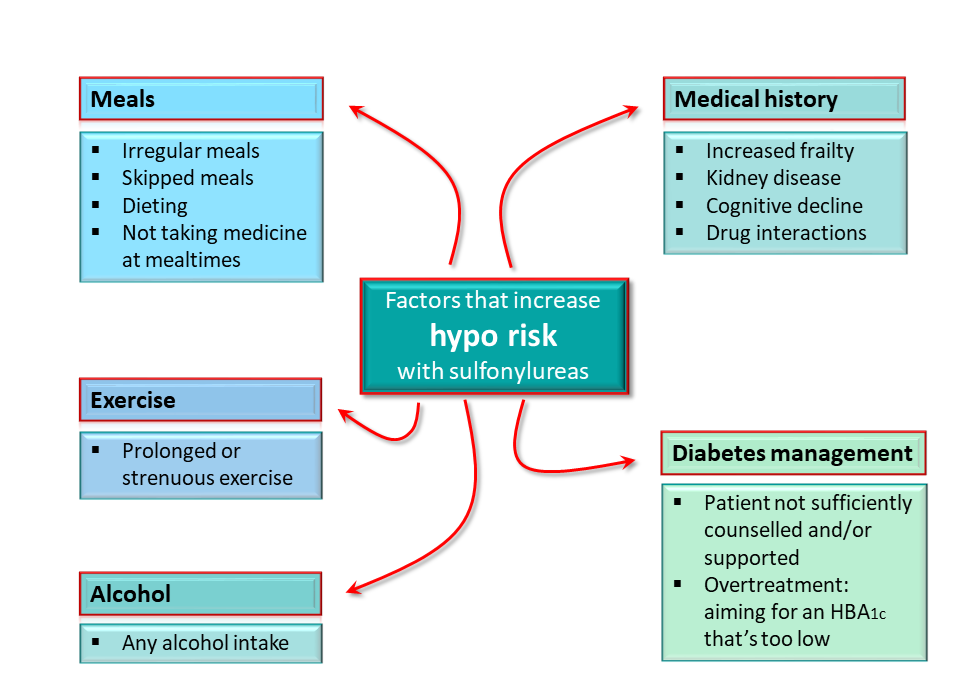
It's important that sulfonylureas are taken just before or with a meal. If no meal is eaten, there will be no postprandial glucose surge to counterbalance the insulin release triggered by the sulfonylurea, potentially causing a hypo. This could happen in nursing homes, for example, if meals don't coincide with the time when a sulfonylurea dose is given. Hypo risk is also elevated when a patient reduces their overall daily food intake whilst continuing on the same dose of a sulfonylurea. This situation may arise if a patient starts dieting – especially a low carbohydrate diet – or skips meals because they are preoccupied. Some older patients in cognitive decline may forget to eat.
Alcohol or more exercise than normal may exacerbate the hypoglycaemic effects of sulfonylureas, especially if inadequate food has been ingested as well.
Patients with cognitive decline may engage in behaviours that increase the risk of a hypo such as eating irregularly, and their behaviour and inability to communicate may make it difficult to detect a hypo until the patient collapses. Hypoglycaemia may also go unnoticed in frail patients who have low body weight and are often under-nourished. Some degree of renal dysfunction is inevitable in older patients, but chronic kidney disease can impair the release of glucose that normally happens as a counter measure to hypoglycaemia and reduces insulin clearance.
In terms of interactions, certain azole antifungals, ACE inhibitors, and NSAIDs are examples of medicines that may enhance the hypoglycaemic potential of sulfonylureas. Refer to the SmPCs for each drug for more details.
The risk of hypoglycaemia can be increased if prescribers aim for an HbA1c target which is too low. The Association of British Clinical Diabetologists suggest that the older patient's overall health, cognitive and functional status should be taken into account to establish an individual glycaemic target. In the absence of robust clinical trial data, they suggest an HbA1c target of 7 – 8% (53 – 64mmol/mol) for patients with mild to moderate frailty. For severe frailty, a target range of 7.5 – 8.5% (59 – 69mmol/mol) is suggested.
Finally, as we saw in the opening case study, patients who have not been educated properly about managing diabetes or who are not sufficiently supported are more at risk of developing problems.
⇦ PREVIOUS PAGE – Page 4 of 6 – NEXT PAGE ⇨